Achilles paratenon issues are challenging. They often don’t respond to our interventions. This is probably because paratendinitis is not very common. We have not yet developed a good understanding of how to manage it. (having said that, some would say the same for Achilles tendinopathy!).
So what is paratendinitis? It is inflammation of the paratenon (or sheath) of the Achilles tendon. Inflammatory fluid develops in the tendon sheath. This can be very minor and only on one side of the tendon (medial or lateral). Or in more severe cases it can go all the way around the tendon.
It is different to a thickened paratenon which occurs in people with a very thick and pathological Achilles tendon (the structure-dominant people in Shawn Hanlon’s subgroups). Most people with a true paratenon issue have minimal or no tendon pathology.
The symptoms are different to Achilles tendinopathy. Often people get more diffuse symptoms up and down the tendon. Having said that, I have seen very localised pain from the paratenon on either the medial or lateral side of the tendon that fits exactly with the site of a small amount of paratenon fluid. Not as common. People with a substantial amount of fluid can also get crepitus.
The other thing you will see is a non-proportional load to pain relationship. Most (definitely not all) people with tendinopathy report higher pain as you progress for activities that load the tendon a little to activities that load the tendon a lot (e.g. going from a double leg calf raise to a hop). Among people with a paratenon issue the load-to-pain relationship is not like this. They tend to report the same pain regardless of load.
This poor load-to-pain relationship is explained by the drivers of injury and the tissue injured. What I have observed in the clinic over the last few years is that some (not all) of these seem to be driven by a biomechanical factor. They seem to have excessive foot pronation on high demand stretch-shorten cycle tasks like repeated hops, especially as they fatigue (get them to repeat the hop for 30 seconds). This could cause greater shear forces between the tendon and paratenon that is designed for sagittal plane loading.
Here is a video of someone hopping. Notice the pronation in the load absorption phase. Note, it is not a great example. I will try and find a better one. I forget to video the really good ones!
Write your awesome label here.
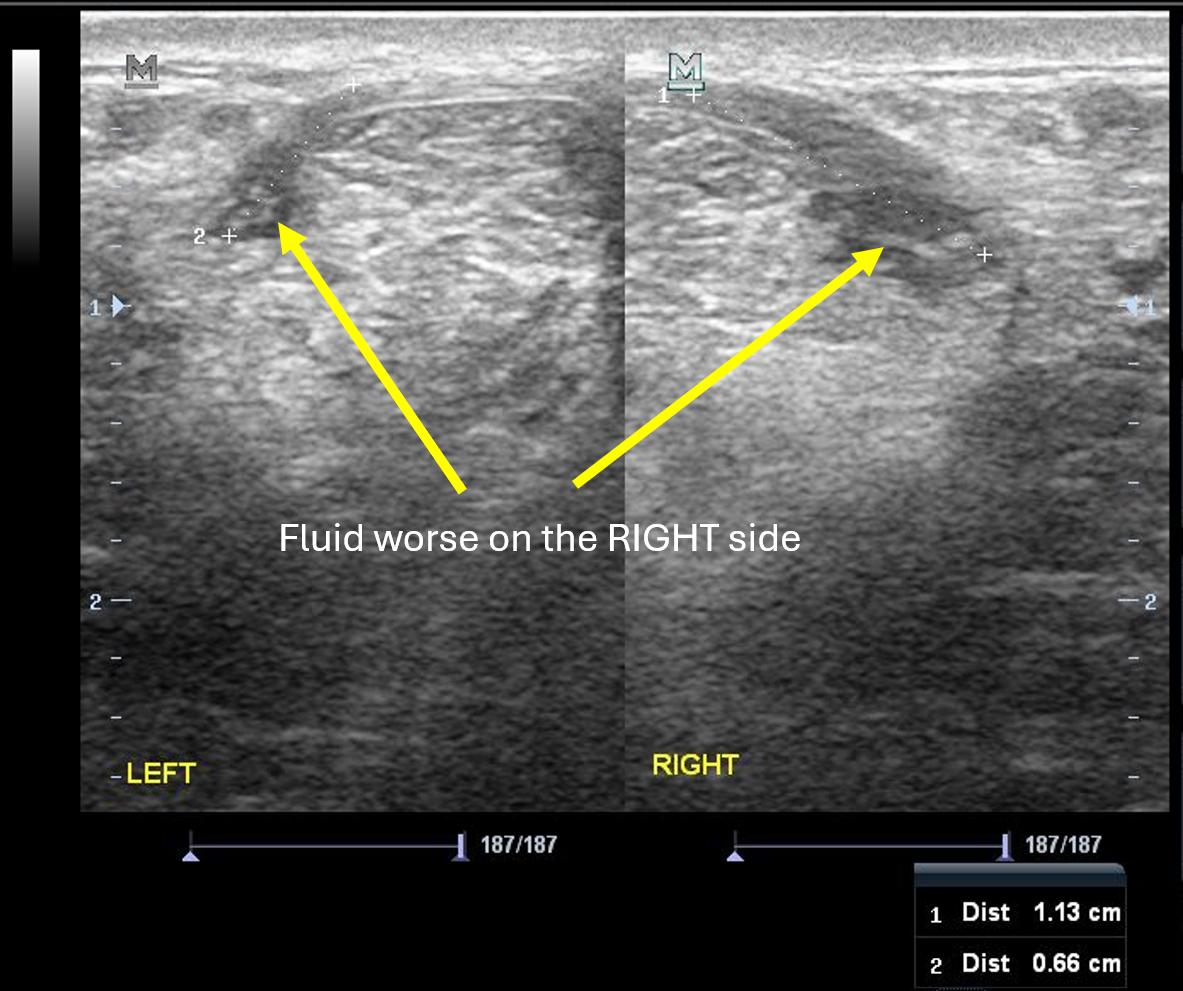
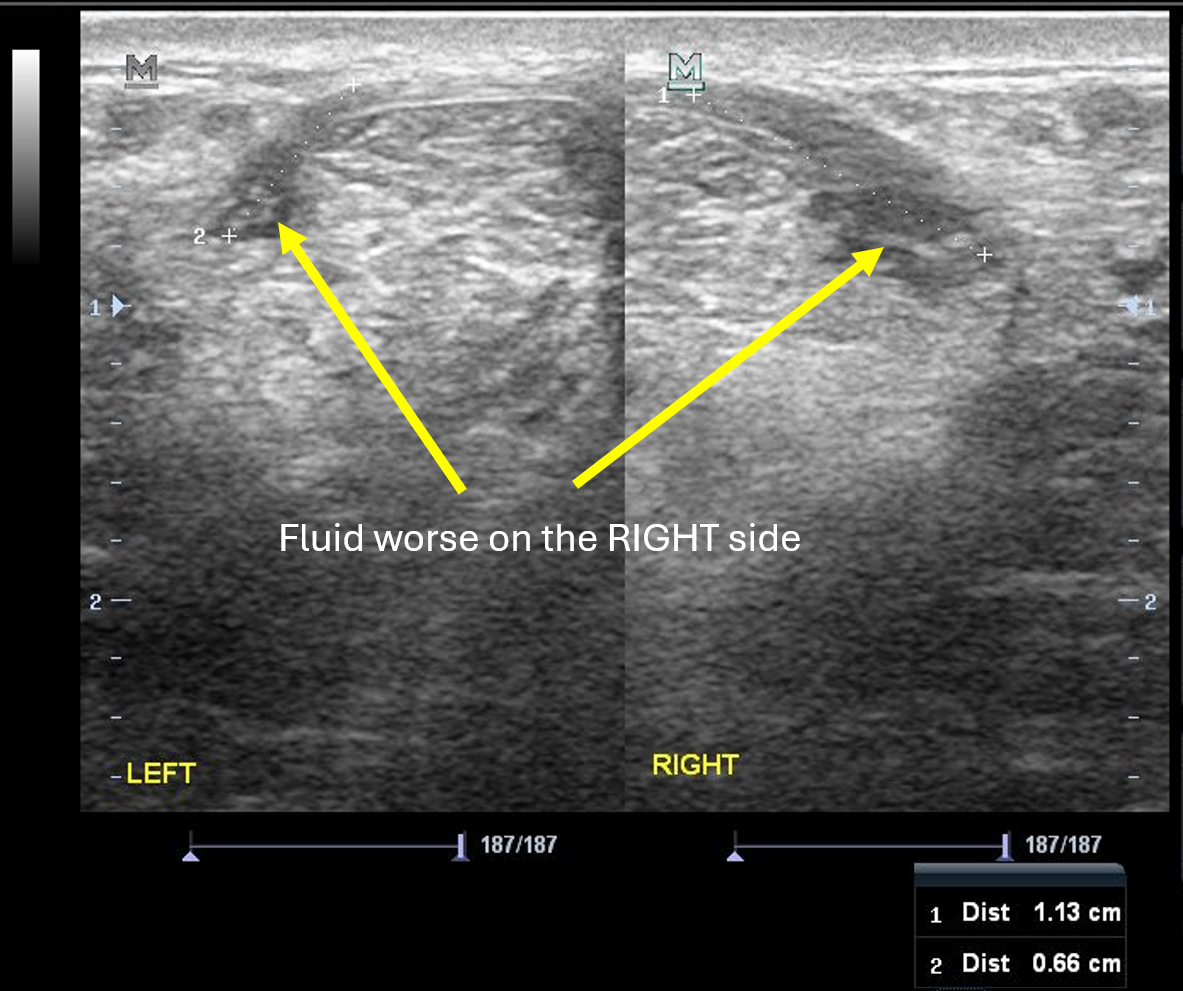
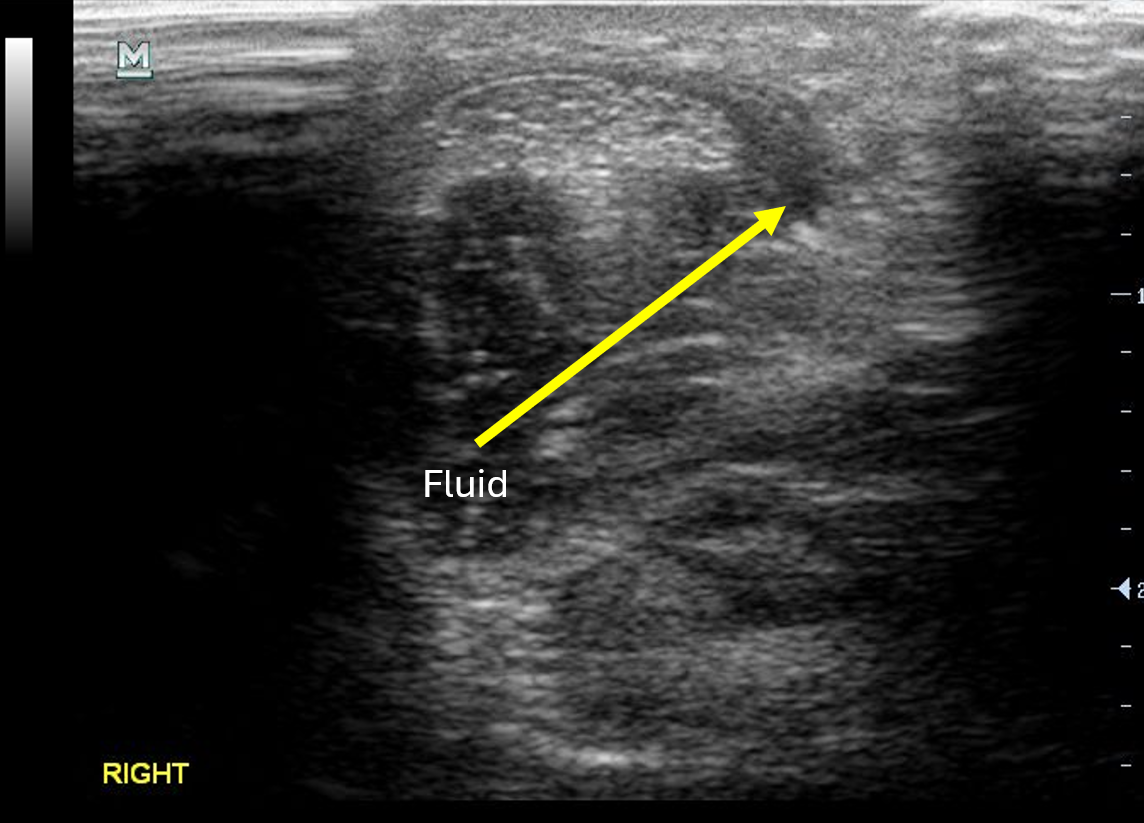
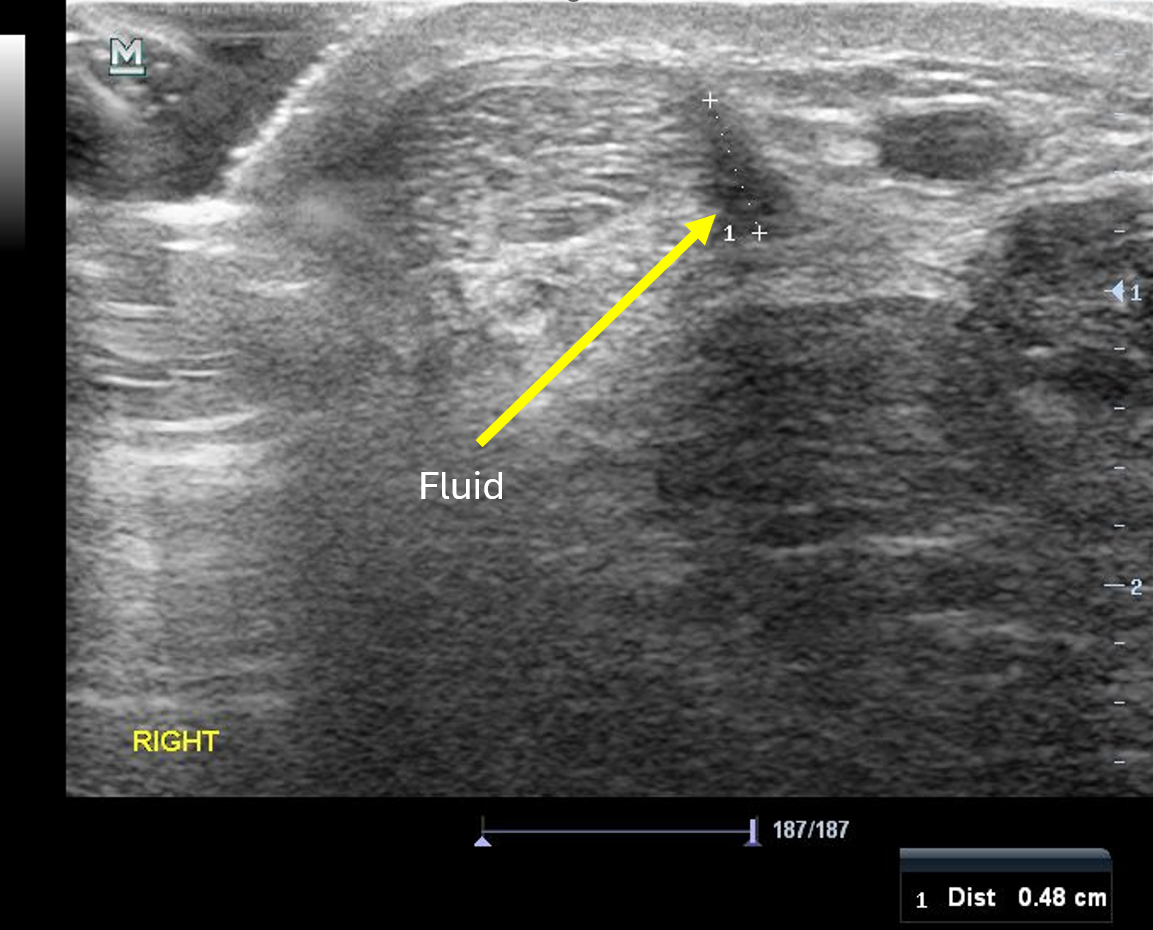
And here are some ultrasound images showing paratenon issues. These are from three separate patients. Each had minimal or no tendon changes and paratenon fluid on the lateral > medial side of the tendon. There are also measures of the size on the longest dimension for two of them.
What I make sure I do with these people is assess dynamic pronation in walking, running, hopping in various ways (rested, fatigue, maximal, forward, etc). If this is a feature, my go to is strength and capacity in the tissues followed by stiffening of the foot lever during dynamic SSC tasks (maximising efficiency of sagittal plane stretch shortening cycle and minimising ‘leakage’ into pronation).
Just putting this out there as I have not heard people mention it prior. Would love to your thoughts and personal experienced related to this.