This blog is about Achilles tendon tears. Although they are rare, they are real!
if you are in the Gold Coast or UK, my new course is coming your way!
Details here: https://www.tendinopathyrehab.com/clinicians-offering or click here
There’s ongoing debate about whether Achilles tendon partial
tears truly exist. I’ve seen a few recently, ranging from elite to
recreational athletes and people who just walk.
These injuries usually happen on the background of
pre-existing tendon issues, most commonly midportion Achilles tendinopathy.
Typically, there’s a sudden force or injury that causes tissue breakdown,
similar to a muscle strain (which is also a tendon/soft tissue problem).
Importantly, this type of acute tear is different from a
radiology report describing a “tear,” “delamination,” or “split” within the
tendon. Without a good history, we can’t be sure how those findings developed (and
even with a detailed history, we’re sometimes still not sure).
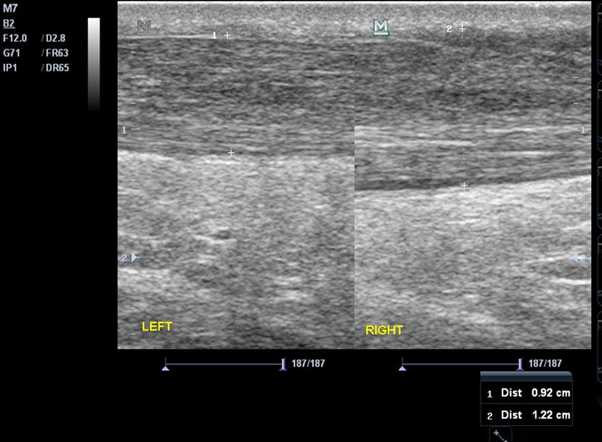
Anyway, here is an interesting recent case of a partial
Achilles tear. Was treating him for midportion symptoms on the RIGHT side,
although he had some minor symptoms on the LEFT as well. The image below shows the
midportion on each side before the tear incident. The LEFT, more symptomatic
side is much thicker but both have changes to the collagen fibrillar structure.
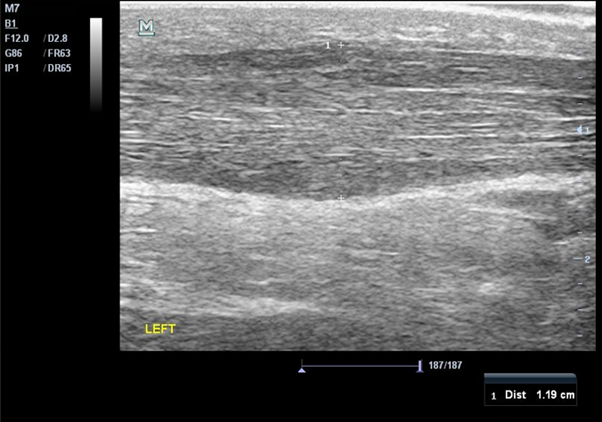
So, then he had his incident. He was feeling better with
some initial rehab on the RIGHT so against advice played soccer with
friends. During the second game the LEFT Achilles was sore, but he continued.
Then something happened, an incident, major pain and he had to stop. He presented
to me 1 week later. You can see the LEFT tendon was now 30% thicker front to
back (anteroposterior).
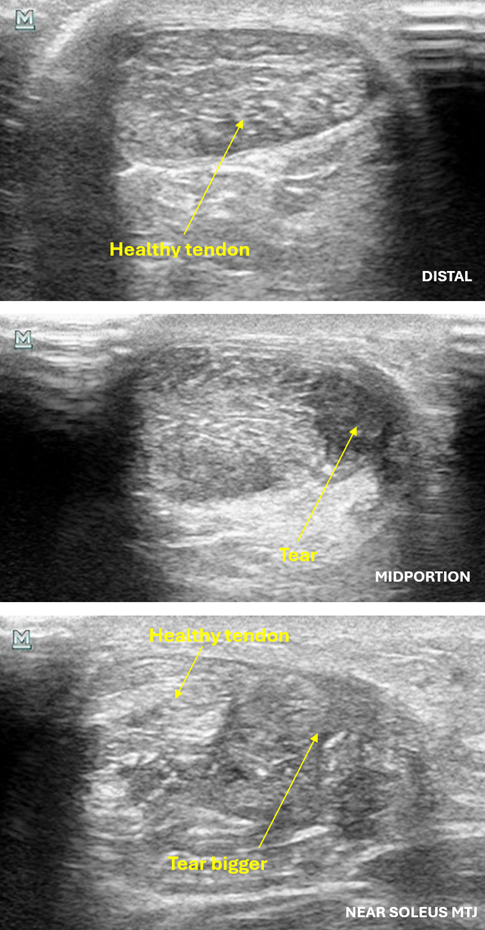
And the image below shows the tear on the medial side of the
Achilles (soleus sub- tendon?) and as we move from distal to proximal the tendon
is more affected.
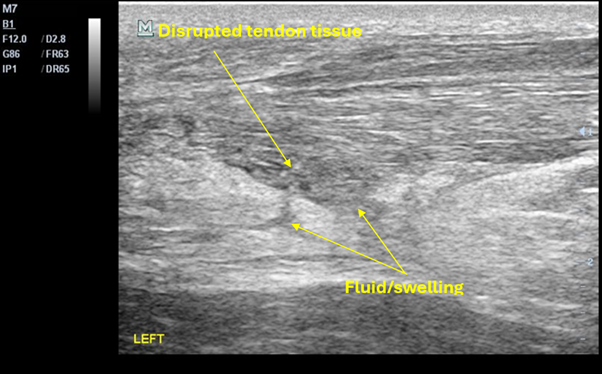
And the last image shows the tear in the longitudinal plane at about the level of the soleus MTJ.
Interestingly, the Achilles tendon resting angle was different but only with knee bent, indicating soleus resting tension was reduced.
The good thing is no need for surgery or a boot (as long as appropriate footwear is worn). He is now progressing well with the right rehab.